

Knowing when to refer a patient to step-up care for eating disorder treatment can be challenging for providers. Many eating disorder patients do not present in a way that makes escalation obvious. Some remain medically stable while deteriorating psychologically. Others may engage in outpatient care but show minimal progress with increased rigidity, nutrition instability, or symptom worsening. One of the most important provider decisions, then, is recognizing when a patient needs more structure than weekly outpatient support.
Understanding the Continuum of Eating Disorder Treatment
Before reviewing the clinical indicators that suggest a patient may benefit from a partial hospitalization program (PHP) or intensive outpatient program (IOP), it’s important to understand how these levels of care fit within the broader eating disorder treatment continuum.
The American Psychiatric Association (APA) emphasizes that level-of-care decisions in eating disorder treatment should be based on more than diagnosis alone. Factors such as medical stability, psychiatric symptoms, nutritional status, motivation for recovery, prior treatment response, and available psychosocial support all influence the most appropriate care setting. Additionally, referral considerations may differ for adolescents, particularly when family involvement and developmental needs shape treatment planning.
Generally, outpatient care is appropriate for medically stable patients who show progress with lower-frequency intervention. IOP provides increased structure and therapeutic support for patients who need more than traditional outpatient care while maintaining some daily responsibilities. PHP offers intensive daily treatment for patients who require greater clinical oversight without inpatient hospitalization. Residential or inpatient care may be necessary when symptom severity, psychiatric acuity, or medical concerns require a higher degree of supervision and support.
Eight Signs Outpatient Care May No Longer Be Enough
Below are eight clinical indicators that a patient may benefit from a higher level of care beyond traditional outpatient treatment. It’s critical to remember that medical stability alone does not rule out the need for a higher level of care, particularly when behavioral symptoms or psychological distress are intensifying.
- Persistent restriction, bingeing, purging, compulsive movement, or other compensatory behaviors despite outpatient treatment
- Weight loss or failure to progress toward nutritional restoration goals
- Increasing meal-related distress or inability to complete meal plans independently
- Escalating anxiety, depression, obsessive-compulsive disorder (OCD) symptoms, or emotional dysregulation
- Frequent cancellations, treatment avoidance, and/or low engagement
- Family conflict or caregiver burnout that impacts progress
- Functional decline in school, work, and/or relationships
- Repeated relapse after lower-acuity treatment
When PHP Is the Right Referral: Structured Daily Intervention
PHP is often considered the “middle ground” between outpatient treatment and inpatient hospitalization. Recent research examining eating disorder partial hospitalization programs suggests that structured, multidisciplinary day treatment can support meaningful improvements in symptom severity among patients who need more intensive intervention than outpatient care alone can provide.1
PHP may be appropriate when a patient:
- needs daily therapeutic support
- requires supervised meal times
- needs multidisciplinary intervention, including therapy, psychiatry, and nutrition
- has not responded well to outpatient or IOP care
- is medically stable enough to avoid hospitalization
When IOP May Be Appropriate: More Support Without Full-Day Treatment
IOP often serves as either a treatment intervention or a step-down support. Emerging research continues to reinforce the value of structured higher levels of care for eating disorders, particularly when outpatient treatment alone is not producing sufficient progress. Recent findings suggest that intensive multidisciplinary programs can meaningfully reduce eating disorder symptoms while supporting broader emotional and functional recovery.2
IOP is a good fit for patients who:
- need more than weekly outpatient care to reduce eating disorder behaviors or reinforce treatment goals
- benefit from structured meal support and real-time therapeutic intervention around eating-related distress
- are stepping down from a PHP or residential program and still require consistent support
- can maintain relative medical and psychiatric stability between sessions
- continue to experience restriction, binge eating, purging, compulsive movement, or other compensatory behaviors, but do not require daily full-day treatment
- struggle with treatment adherence in traditional outpatient settings, including difficulty following meal plans or using coping strategies independently
- experience moderate difficulties in work, school, family, and/or social functioning, but can still participate in aspects of daily life
- would benefit from multidisciplinary care coordination, including therapy, nutrition support, and psychiatric oversight
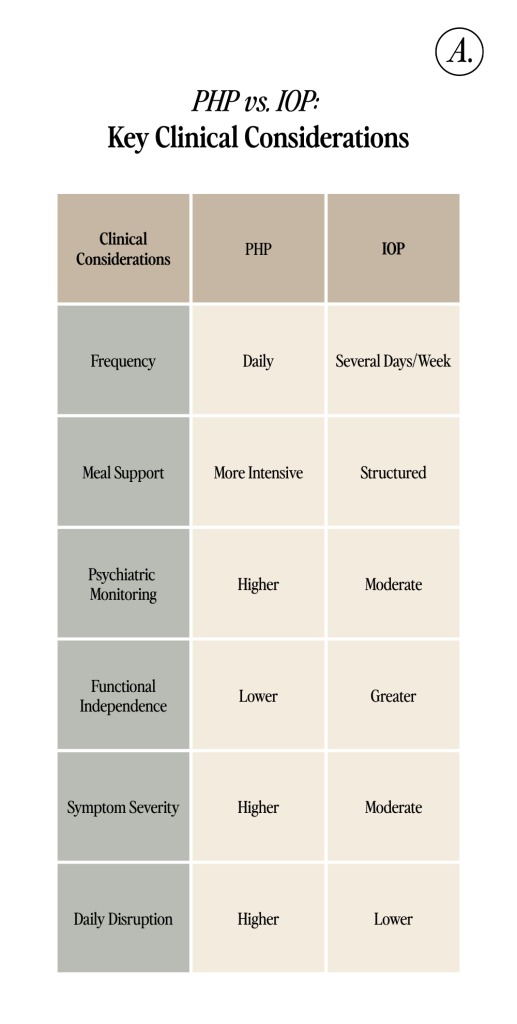
PHP vs. IOP: How to Think About the Difference
While PHP and IOP both provide structured multidisciplinary eating disorder treatment, the appropriate referral depends on symptom severity, required structure, and the patient’s ability to function between sessions. In general, PHP is better suited for patients who require daily intensive intervention and greater clinical oversight, while IOP may be appropriate for patients who need more support than traditional outpatient care while maintaining aspects of daily life.
Refer Your Patients to Alsana with Confidence
Ultimately, knowing when to refer a patient to PHP or IOP can make a meaningful difference in both short- and long-term recovery outcomes. Alsana offers specialized programming designed to meet patients where they are in recovery with individualized, Soul Hearted care across the treatment continuum.
Visit our website to learn more about our in-person and virtual treatment options for adolescents and adults or to refer a patient.
References
- Rubenson, M. P., Gurtovenko, K., Simmons, S. W., & Thompson, A. D. (2024). Systematic review: Patient outcomes in transdiagnostic adolescent partial hospitalization programs. Journal of the American Academy of Child & Adolescent Psychiatry, 63(2), 136–153. https://doi.org/10.1016/j.jaac.2023.03.022
- Reilly EE, Gorrell S, Duffy A, Blalock DV, Mehler P, Brandt H, McClanahan S, Zucker K, Lynch N, Singh S, Drury CR, Le Grange D, Rienecke RD. Predictors of treatment outcome in higher levels of care among a large sample of adolescents with heterogeneous eating disorders. Child Adolesc Psychiatry Ment Health. 2024 Oct 17;18(1):131. doi: 10.1186/s13034-024-00819-8. PMID: 39420352; PMCID: PMC11488273.

